35/M with pedal edema and SOB
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio.
Case history:
A 35/M came with the complaints of SOB since 3 days and pedal edema since 5days.
SOB (grade - II) was insiduous in onset, aggravated on sleeping, relieved in sitting position. He had similar complaints of SOB (in aggravated state) and got admitted in a hospital during the 1st lockdown of covid.
Pedal edema - it was insiduous in onset, gradually progressive, pitting type in B/L lower limbs.
Patient used to work in petrol bunk and quit working 7 months back and now stays home. During which, he started drinking toddy of 1500ml/day everyday. He had a history of alcohol consumption (1 quarter) on a daily basis until last 6months(since 10years). He also has smoking history of 1packet/2 days since 10 years.
Past history:
▪ N/K/c/o DM, HTN,TB.
▪ No history of CVA, asthma, epilepsy, CAD.
Family history
Not significant
Personal history
* Diet- mixed.
* Appetite- normal
* Sleep- adequate
* bladder movements - regular
* Bowel movements- regular
* addictions - alcoholic, smoking since 10years.
General examination:
Patient was conscious , coherent, cooperative well oriented to time , place person
Pallor- absent
icterus- absent
cyanosis- absent
clubbing- absent
Lymphadenopathy - absent
Edema- B/L pedal edema present.




Vitals:
Temp: 98.6 F
BP: 120/70 mm Hg
PR: 74 bpm
Spo2: 100% @ RA
Systemic examination;
RESPIRATORY SYSTEM-
Inspection-
Chest is bilaterally symmetrical
The trachea is positioned centrally
Apical impulse is not appreciated
Chest moves normally with respiration
No dilated veins, scars or sinuses are seen
Palpation-
Trachea is felt in the midline
Chest moves equally on both sides
Apical impulse is felt in the sixth intercostal space
Tactile vocal fremitus- appreciated
Percussion-
The areas percussed include the supraclavicular, infraclavicular, mammary, axillary, infraaxillary, suprascapular, infrascapular areas.
They are all resonant.
Auscultation-
Normal vesicular breath sounds are heard.
Per Abdomen
Inspection:
Skin - regular, normal.
Shape - distended
Umbilicus - normal
Abdominal wall movements - present
No visible pulsations and peristaltic movements seen.
Palpation:
Tenderness - mild in right hypochondrium,
No rise of temperature
Liver - palpable mildly.
Spleen - not palpable
Percussion:
Liver - dull note
Spleen - dull note
No shifting dullness, fluid thrill.
Auscultation:
Bowel sounds heard.
No bruit.
CARDIOVASCULAR SYSTEM-
Inspection-
The chest wall is bilaterally symmetrical.
No dilated veins, scars or sinuses are seen
Apical impulse or pulsations can be appreciated in sixth intercostal space 2cms lateral to mid clavicular line
Palpation-
Apical impulse is felt in the sixth intercostal space, 2 cm away from the midclavicular line
No parasternal heave or thrills are felt
Percussion-
Right and left borders of the heart are percussed
Auscultation-
S1 and S2 heard, no added thrills and murmurs are heard
Central nervous system:
No abnormalities detected
Investigations:
Serology - negative
BGT - O positive
RBS -141mg/dl
Sr. Urea -32mg/dl
Sr. Creatinine -0.8mg/dl
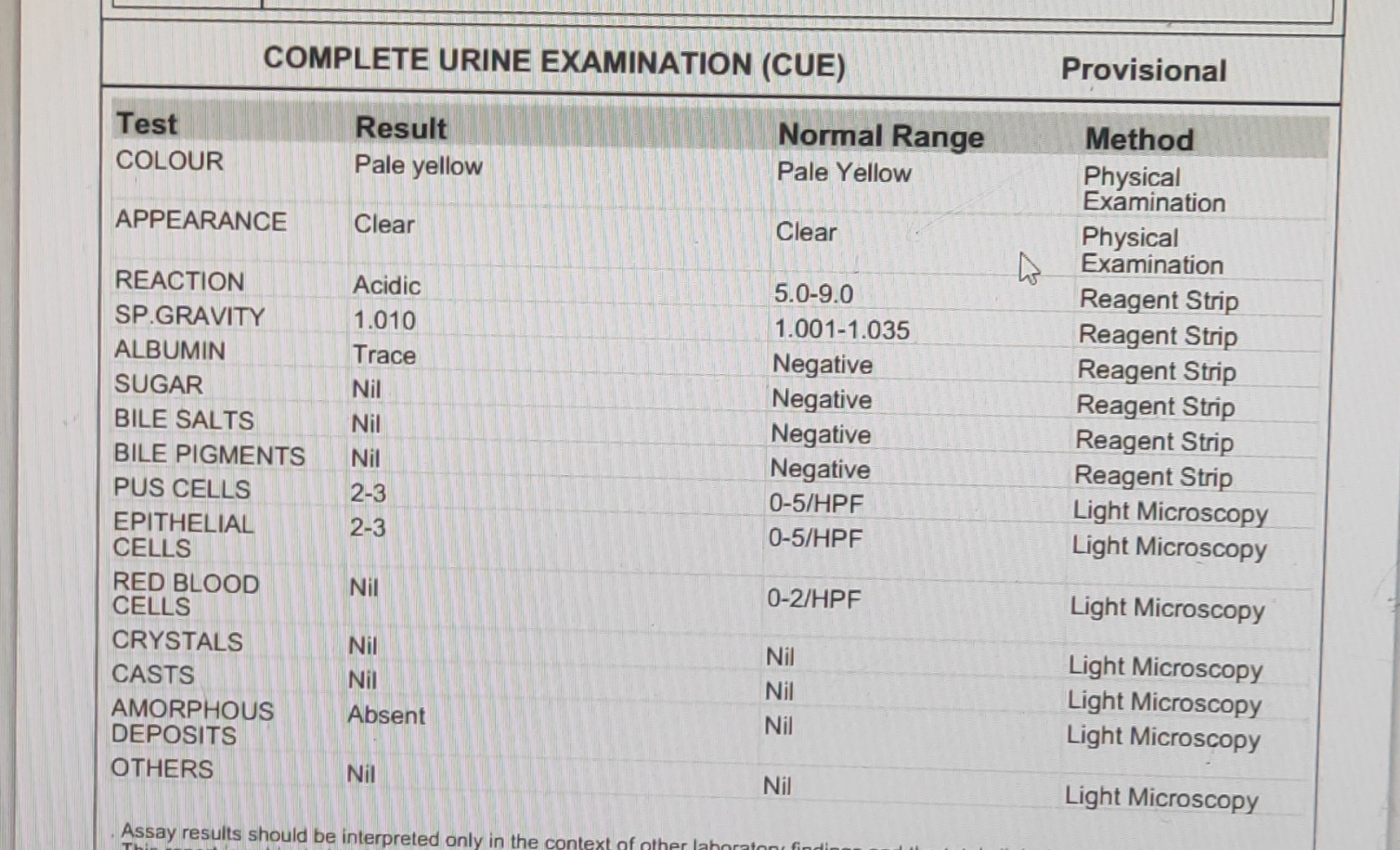
CUE
ECG

Hemogram

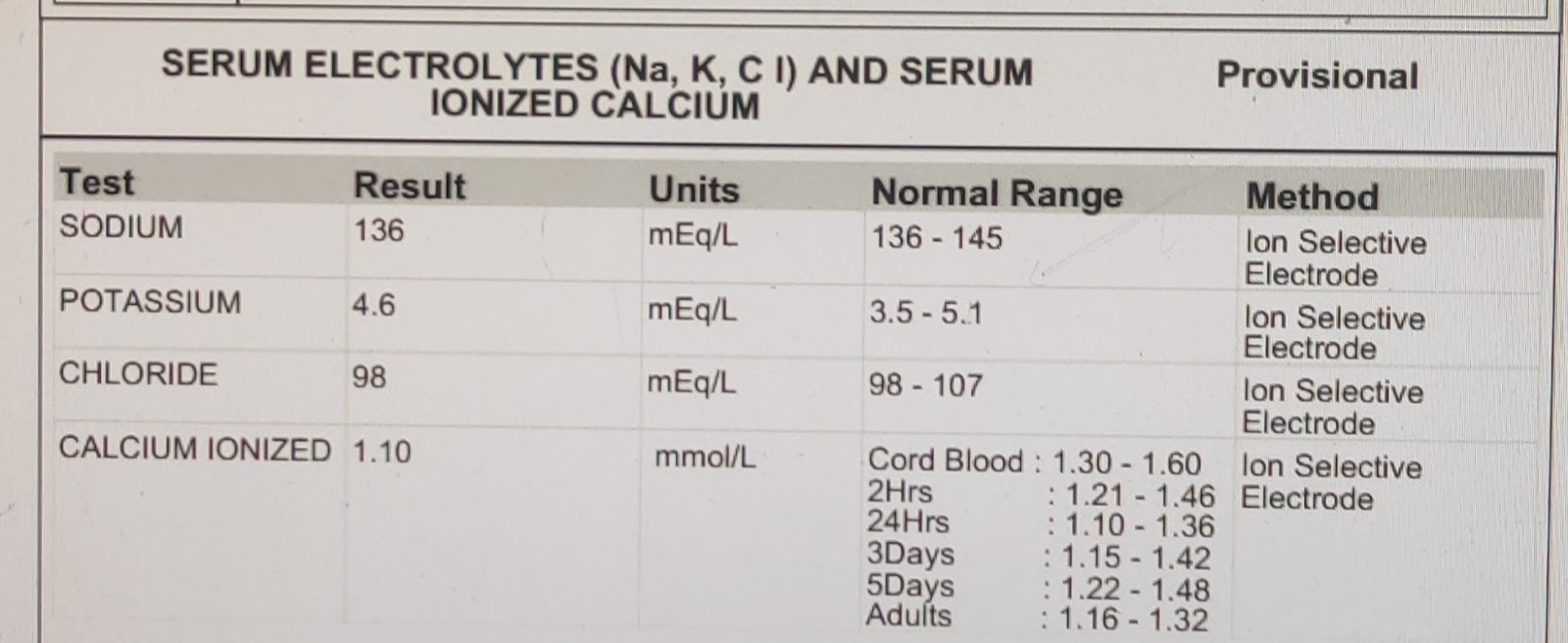
Sr. Electrolytes
Chest Xray




Comments
Post a Comment